Wrist passageway syndrome or carpal tunnel syndrome is the most common narrowing neuropathy. It’s a median nerve laceration on the inside of the wrist. It is manifested by altered sensation, numbness and deadness of the first three fingers on the hand, as well as burning pain in the area of the wrist and can spread upwards towards the elbow and shoulder.
When problems arise, we like to help ourselves by shaking hands, which slightly alleviates the symptoms. The pain can get worse at night and is sometimes so intense that it interrupts sleep.
Let’s look at what’s going on in the wrist that causes such difficulties, and we’ll try to answer questions about how to get a diagnosis of carpal tunnel syndrome (CTS), what to do when symptoms are already present, whether surgery is always needed, and what we can do if our daily activities are among those that lead to the development of problems.
Carpal tunnel anatomy
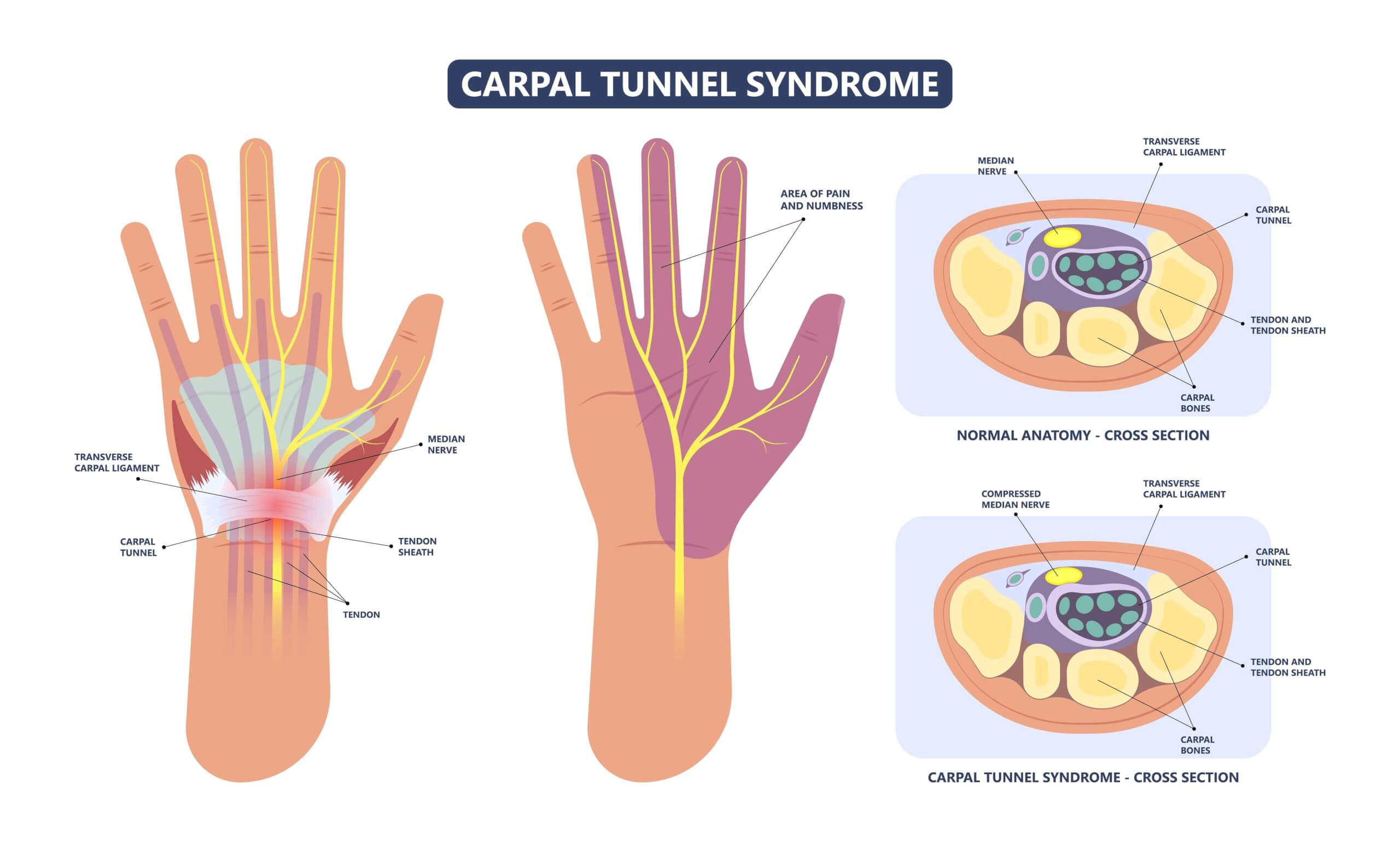
There are many small bones in the wrist, and through them, an even greater number of muscles, tendons and ligaments participate in the precise movement of the wrist and fingers. In the wrist there are 8 small bones are classified into two rows, called carpal bones. The bones are shaped to form a “carpal canal” on the inside of the wrist. It is a narrow passage with many independently moving structures.
Among them, there are as many as nine flexor tendons, there is also an important nerve (nervus) medianus. This is located, not exactly in the middle of the wrist (carpal tunnel), but slightly towards the thumb side. The transverse carpal ligament runs transversely across the wrist and n.medianus in the carpal canal runs below it.
If we compare it with the ulnaris nerve, which resuscitates the 5th finger and travels above the ligament outside the carpal canal, we can see that when the carpal canal structures are compressed, there is no simultaneous compression of the n.ularis, and thus the pinkie remains unaffected. Muscles affected by carpal tunnel syndrome are mainly thumb muscles, so at higher levels of CTS, visible atrophy of the thenar is noticed – i.e. a cluster of thumb muscles (4).
Who is most commonly diagnosed with wrist passage syndrome
Carpal tunnel syndrome (CTS) is the most common constriction neuropathy, accounting for as much as 90% of all. It occurs due to increased pressure or inflammation in the area of the carpal canal, affecting the nerve that passes through. The most common cause of occurrence is repetitive movement in the wrist, which includes typing, working with machines, or prolonging the static posture of the wrist in flexion or extension, such as holding a computer mouse, car steering wheel, etc.
Genetic predisposition and obesity, increased thyroid function, and certain autoimmune diseases, such as rheumatoid arthritis, can also contribute to the development of CTS. Diabetes increases the prevalence of the occurrence of CTS by 80% and is thus an important factor in the occurrence. The syndrome also occurs several times during pregnancy or during the menopausal period, due to hormonal changes in the female body (3).
According to studies, women are expected to experience CTS as much as 3 times more frequently than men.
Causes of carpal tunnel syndrome
Carpal tunnel syndrome usually occurs as a result of a combination of compression and traction – i.e. squeezing and stretching. The compression part includes a complete cycle in which the blood supply is inhibited due to increased pressure or compression, local oedema is increased and n.medianus intra-neural microcirculation is compromised.
In doing so, the nerve function and structural integrity of the nerve itself become compromised. A dysfunctional environment contributes to the inflammation of connective tissues around them, thereby losing normal function, which is in the first order protective and supportive. Inflamed tendons, that travel through the carpal canal, can compress the n.medianus.
The other problematic part is repeated pulling (traction) and movement of the wrist, which additionally contributes to a negative environment and damages the nerve.(1)
Symptoms
The wrist-pass syndrome is recognized by altered sensation, which is described as numbness and deadness. The first three fingers are affected and the second half of the fourth finger is affected. The burning pain initially occurs at night, and then the pain episodes increasingly occur during the waking hours.
The condition gets worse at static wrist postures – either in flexion or extension. The sense of touch and fine motor skills are deteriorating. Those who experience symptoms often explain that they have difficulty buttoning and picking up small things with their fingers.
Muscle weakness of the thumb is also noticed, which is observed as visible muscular atrophy in the advanced state (3).
Diagnosis
The above-described sequence of symptoms is extremely typical for the diagnosis of carpal tunnel syndrome and rarely occurs in other disorders. Therefore, the clinical presentation is the most important element in determining the diagnosis.
There are also two clinical tests that help determine the diagnosis, and these are Phalen and Tinel tests. In a positive Tinel test, by gently tapping the affected site of the median nerve, we provoke tingling and stinging. In a positive Phalen test, however, by maintaining a 90° flexion or extension of the wrist for 30-60 seconds, we induce symptoms of CTS – i.e. pain, stinging, tingling, etc.
We use EMG (electromyography) method to measure nerve conduction rate (4) to determine the degree of defect.
Conditions with similar symptoms
Which conditions can cause similar symptoms but are not carpal tunnel syndrome (CTS)?
One of the conditions that could be mistaken for CTS is cervical radiculopathy – compression of the nerve roots in the neck area, which is manifested in sensory and motor disruptions in the arm. A thorough clinical examination conducted by an expert, an EMG and diagnostic imaging of the cervical spine is an important method when another condition is suspected to be the cause of problems.
Osteoarthritis, which may cause similar pain, should also be considered, however, neurological symptoms are not usually present with that condition (3).
Treatment options for carpal tunnel
Treatment depends on severity of the condition, individual problems and personal preferences. It is advised that mild to moderate CTS be treated non-surgically, whereas moderate to severe CTS be treated surgically.
Your physiotherapist must explain to you your condition and the course of rehabilitation. CTS is usually a long-term condition, so you will need to be patient with your treatment.
It is important you know this, so that there is no confusion as to why, after a week, the condition is not gone. Treatment lasts for months, not weeks.
Non-surgical treatment
Non-surgical treatment is a treatment that uses a variety of methods, approaches and devices but does not involve surgery.
You can try the methods described above, i.e. lifestyle changes, adjustments to the working environment, and wrist braces. Perform exercises to strengthen the fingers and muscles of the wrist. Specific neuro-dynamic exercises will help with correct nerve gliding. As far as therapy with medical instruments is concerned, therapies with deep ultrasound and pulsed ultrasound methods have had some positive results.
After use, reports have shown reduced pain and sensory disturbances, as well as improvement in the speed of conduction through the nerve fibers (2).
Corticosteroid injections into the carpal tunnel are a common treatment. According to research, they bring short-term improvement within 1–3 months. However, current studies show that these injections are not better than surgery. What is more, they can cause side effects if injected too frequently (1).
Surgery
No one wants to “go under the knife” right away. However, in some cases, prolonged non-surgical treatment without improvement does no good and can worsen the situation. A detailed assessment of your specific condition is crucial because only then can appropriate advice be given. Some signs that surgery is necessary are:
severe muscle loss,
sensory and motor deficits,
severe persistent pain.
In such cases, corticosteroid injections are not usually advised. Instead, surgery is suggested to decompress the nerve and release it. Surgery can be performed either conventionally, by making a longitudinal incision in the wrist, or endoscopically, which means introducing a special instrument to release the nerve inside the carpal tunnel (3).
General advice
Certain daily activities and inactive lifestyles can worsen the condition or slow down the healing process. General advice would be to try to reduce activities that contribute to the inflammatory process or biomechanical stress in your wrist. In order to help with the rehabilitation, it is important to get enough sleep, have a good diet, engage in regular physical activity, and to take care of any other existing conditions and diseases you might have.
If the position of the wrist is the reason for the symptoms, the use of wrist splint isrecommended. It will hold the wrist in a neutral position. You may be bending your wrist unknowingly during sleep, which is then causing you problems. The wrist splint must be used for 3 weeks, at night.
You should also adapt your working environment as well as you can. Keeping the wrist in a certain position for long periods of time may cause problems. A computer mouse that ensures that the wrist remains in a neutral position is recommended for office workers. There are also various mouse pads that provide support for the forearm or wrist. Another option is orthopaedic braces.
It is certainly necessary to discuss with an expert what causes your problems and when, and then find ways to reduce these activities as much as possible.
Carpal tunnel syndrome rehabilitation at the Medicofit clinic
You will need rehabilitation after the surgery. At Medicofit clinic, we provide pain relief and scar therapy with ultrasound, massage, and manual techniques. We continue with sensory re-education and kinesiotherapy with various exercises, which help improve mobility and gain muscle strength.
It is important to us that your arm becomes functional as quickly as possible so that you can use it normally.