Climber’s elbow refers to pain that occurs on the inside of the elbow. Climber’s elbow is a chronic inflammation of the elbow flexor attachments, most commonly the brachialis muscle group, which attaches to the ulnar tuberosity, and less commonly the biceps muscle group, which attaches to the radial tuberosity. In both cases, we experience severe pain on the front or inner side of the elbow.
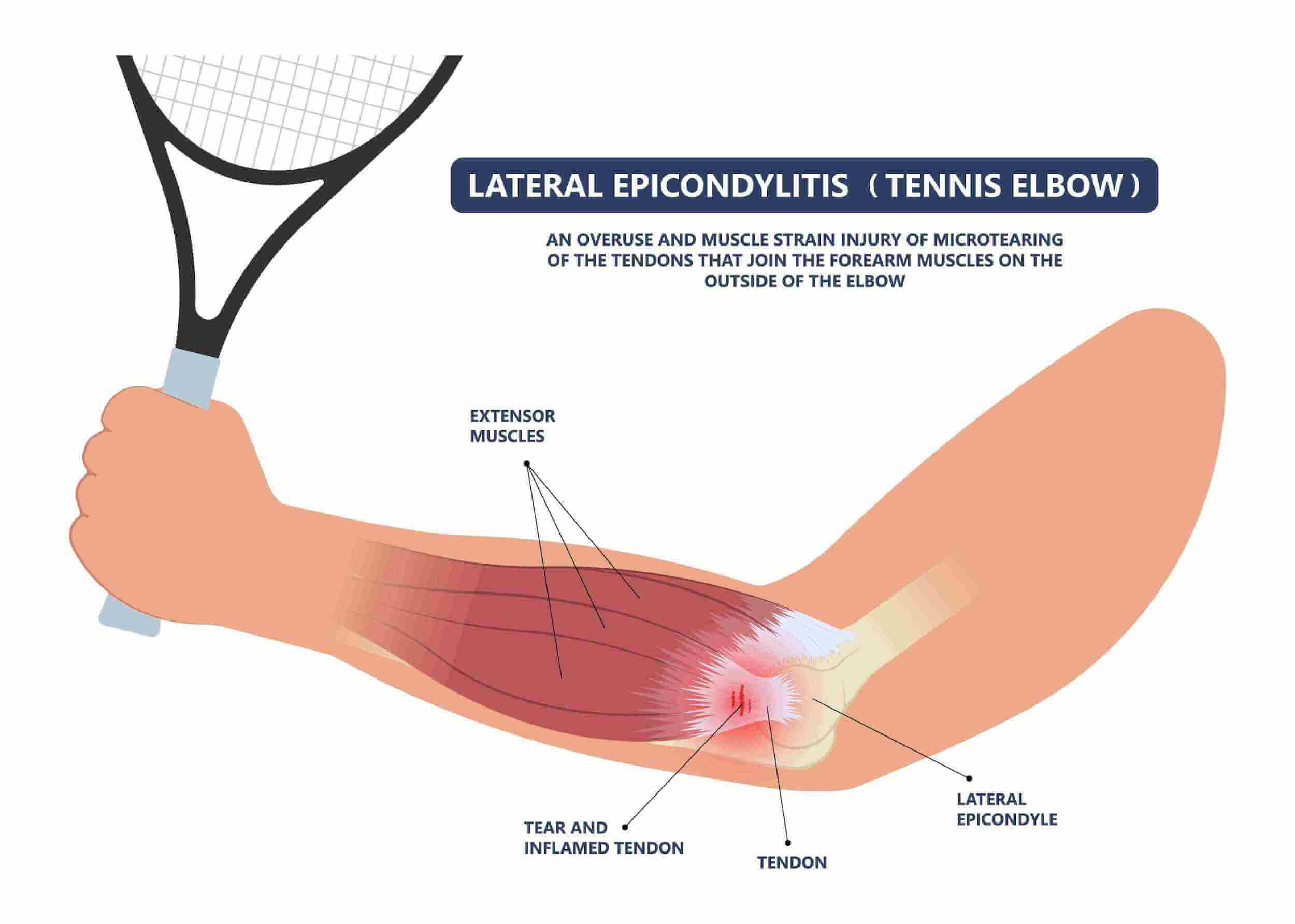
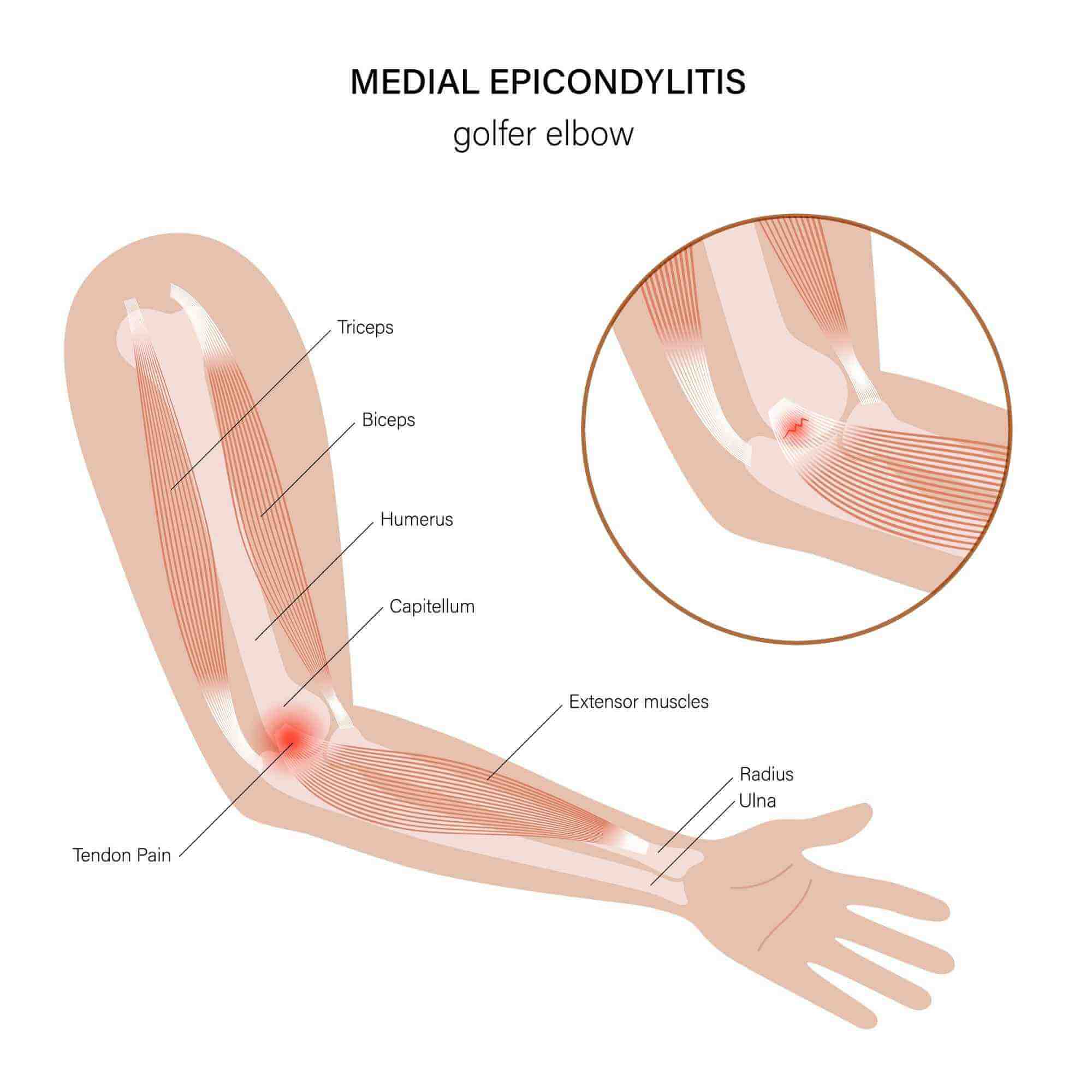
Climber’s elbow is an overuse injury to the tendons of the forearm muscles. Golfer’s elbow and climber’s elbow are not the same pathological condition, although both cases are a tendinopathy. Golfer’s elbow involves inflammation of the tendons of the muscles that flex the wrist, while climber’s elbow involves inflammation of the tendons of the muscles that flex the elbow. In both cases, the pain is on the inner or front side of the forearm, except that in golfer’s elbow it is located slightly higher and more superficially, while in climber’s elbow it is a few centimetres lower and deeper. Overuse leads to degenerative changes in the tendons, which stimulate pain receptors, with the tendons also often in the state of inflammation.
Climber’s elbow is often a chronic condition of climbers, but is not exclusively associated with climbing and the sports population – it is very frequent occurrence in vocations and tasks where above-average load is placed on arms (painting, using a computer mouse, screwing, carrying objects, gardening, vibrations, lifting weights).
Symptoms of climber’s elbow include pain that is burning and sharp, occurs when clenching the fist, lifting loads, and dragging loads with arms, and limits grip strength. The area on the inside of the elbow is often tender, with characteristic unpleasant pain on stronger palpation or manual pressure. Climber’s elbow is characterised by pain spreading from the inside of the elbow down the entire inside of the forearm.
Climber’s elbow occurs primarily due to poor biomechanics of the upper arm muscles, which means that the wrist and elbow positions are incorrect when performing arm movements (the wrong muscle units are overloaded during a particular activity). A frequent cause of climber’s elbow is poor preparation of the forearm muscles for the activities you are performing (the right muscles are overused, but overuse occurs relatively quickly due to poor training; we are talking about poor strength endurance and poor joint mobility). A frequent direct cause of climber’s elbow is muscle asymmetry, which means that the muscles on one side of the forearm are disproportionately stronger or weaker than those on the other side of the forearm (often the muscles on the front of the forearm are stronger and shortened, while the muscles on the back side are relatively weak).
Symptoms of climber’s elbow usually last from 6 to 16 weeks, and if conservative treatment is not performed, the problems can last for several years continuously or in occasional outbreaks of pain, seriously limiting your function. We often resolve cases of elbow problems that have been ongoing for several years because the condition was not treated with training but was mainly focused on pain relief.
Climber’s elbow is treated systematically. First, we perform appropriate diagnostics by measuring muscle properties and look for potential causes of pain in muscle tightness, imbalances, or poor strength. Once we diagnose the causes of climber’s elbow, we perform the appropriate number of treatments to reduce acute pain and prepare the body for subsequent treatment process through training.
The last, key and longest phase of climber’s elbow treatment is individualised kinesiotherapy, which improves the functional muscle imbalances diagnosed during the initial examination and thereby eliminates the primary causes of climber’s elbow. A characteristic of the climber’s elbow pathological condition is that cases where the patient does not persist in the phase of treatment of the causes, i.e. in the muscle strengthening phase, develop recurring elbow problems once the pain subsides. Treatment of an injury is not completed when the symptoms, i.e. pain, disappear. The injury is healed when the causes of the injury are finally eliminated.